

The recently published American guidelines for the management of dyslipidemia reinforce an important shift in how we understand cardiovascular risk. This is not so much about new targets, but about a more precise way of interpreting what is actually happening in each patient.
For many years, dyslipidemia has been understood as an alteration in numbers: elevated LDL cholesterol implied increased risk, and reducing it was the primary treatment goal. While useful, this approach oversimplifies a much more complex process.
Dr. Carlos Martí – Neolife Medical Team
Cardiovascular Prevention
For a long time, the focus has been on identifying out-of-range values. However, we now know that the atherosclerotic process (the accumulation of fat in the arteries) begins long before these values change or symptoms appear.
This explains why some individuals experience cardiovascular events despite having apparently normal blood tests, while others with elevated levels remain stable for years. The difference lies in what is not always visible in conventional testing: particle number, cumulative burden, or the presence of subclinical disease. Today’s tools allow access to this information and enable a better understanding of where each patient stands in the disease process.
The goal, therefore, is not only to detect abnormalities once they become evident, but to interpret earlier signals that allow for more proactive intervention. In cardiovascular health, it is not just about treating risk when it appears, but about understanding how it develops from much earlier stages.
Beyond Cholesterol: Understanding What We Really Measure
LDL cholesterol has traditionally been the cornerstone of diagnosis and treatment. However, not all LDL particles have the same impact, and a normal value does not guarantee low risk. In this context, apolipoprotein B (ApoB) has gained importance. It is a protein present in all particles capable of forming plaques in the arteries, meaning that measuring it is essentially counting how many “potentially harmful particles” are circulating in the bloodstream.
Unlike LDL, which measures how much cholesterol these particles carry, ApoB indicates how many particles are actually present. This is particularly useful in individuals with overweight, diabetes, or elevated triglycerides, where LDL may appear normal despite high risk.
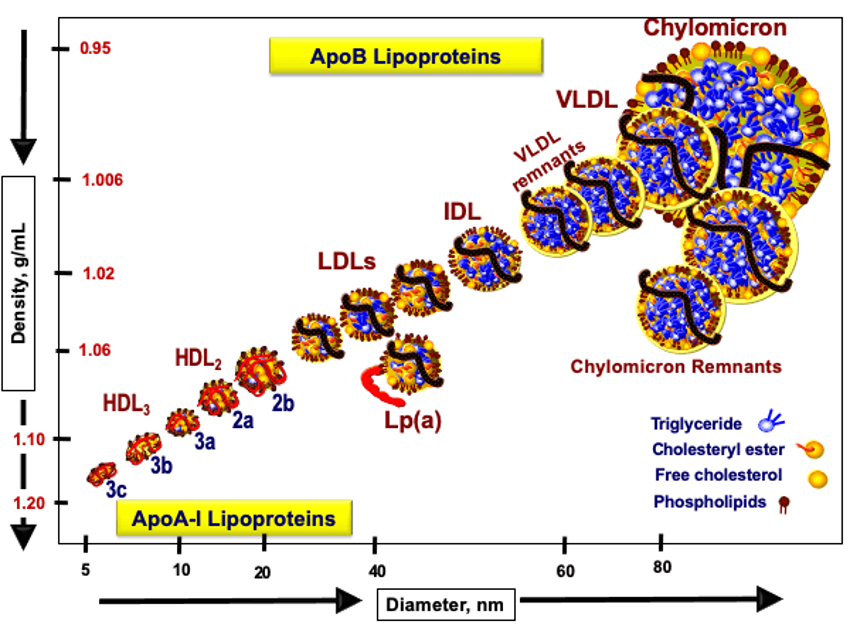
But not all risk depends on lifestyle or metabolism. There is also a genetic component that may go unnoticed in standard blood tests. This is where lipoprotein(a), or Lp(a), becomes relevant. It is a particle similar to LDL but with unique characteristics that make it especially atherogenic (more likely to promote plaque formation in the arteries). Its levels are largely genetically determined, meaning a person may have elevated Lp(a) from birth without knowing it. As a result, even with apparently normal cholesterol levels, cardiovascular risk may be higher than expected if Lp(a) is elevated. For this reason, current guidelines recommend measuring it at least once in a lifetime.
The integration of these biomarkers provides a more comprehensive assessment of risk, moving beyond a model based solely on total cholesterol or LDL.
From Estimating Risk to Detecting Disease
Another key change reinforced by the new guidelines is the use of imaging techniques to refine risk assessment in selected patients. Coronary artery calcium (CAC) measures the amount of calcium deposited in the arteries of the heart. Its presence indicates that atherosclerosis already exists, even in the absence of symptoms.
Although not yet part of the main guideline recommendations, carotid ultrasound allows direct visualization of the neck arteries and the detection of plaques or arterial wall thickening (intima-media thickness, IMT, a marker of arterial health). While CAC identifies more advanced disease, carotid ultrasound can provide information about earlier stages of the process.
At Neolife, these tools are part of an advanced preventive medicine approach. This allows for more precise adjustment of treatment intensity and prioritization of interventions in patients who might otherwise appear low-risk based on conventional testing.
We combine biomarkers such as ApoB and lipoprotein(a) with imaging techniques, including carotid ultrasound, to obtain a more complete picture of vascular health. The goal is not only to estimate future risk, but to determine whether the disease process has already begun—even in its earliest stages.

A More Precise, Not More Complex Approach
The evolution in dyslipidemia management does not mean performing more tests on every patient, but rather selecting more effectively which information is needed in each case.
In practice, this translates into:
- Knowing when a basic blood test is sufficient
- Identifying when measuring ApoB or lipoprotein(a) is useful
- Considering markers such as high-sensitivity CRP (an indicator of low-grade inflammation), which can increase cardiovascular risk even with normal cholesterol levels
- Using imaging tests to clarify uncertainty about actual risk
- Adjusting treatment based on the patient’s overall profile, not just a single value
This approach allows for the identification of high-risk individuals who might otherwise go unnoticed with conventional testing, while also avoiding unnecessary treatment in those who do not need it.
At Neolife, this strategy has long included the assessment of low-grade inflammation, understood as a key factor in the development of atherosclerosis. It is not only about how much cholesterol circulates, but about the environment in which that cholesterol acts.
Applying a Comprehensive Strategy: Addressing the Cause, Not Just the Numbers
Lifestyle interventions remain the foundation of treatment, but their impact goes far beyond lowering cholesterol. Reducing visceral fat (fat stored around organs), improving insulin sensitivity, engaging in strength training and aerobic exercise, and ensuring adequate sleep all directly influence the formation of atherogenic particles, inflammation, and arterial health.
This explains why two individuals with the same cholesterol levels may have completely different risks. The goal is not just to improve lab results, but to modify the metabolic environment in which the disease develops.
Understanding Risk Before It Becomes Visible
Cardiovascular risk does not appear suddenly—it develops progressively over time. We now know that the atherosclerotic process begins long before laboratory values change or symptoms arise. This is why a conventional blood test does not always reflect true risk. Factors such as particle number, inflammation, and subclinical disease can make a critical difference. The real advancement lies in being able to access this information and understand where each patient stands in the process, allowing for earlier and more effective intervention.
At Neolife, this approach is part of daily clinical practice: integrating advanced laboratory testing, biomarkers, and vascular imaging to detect risk before it becomes clinically apparent and to address it in a personalized way.
Because in cardiovascular health, the goal is not simply to act in time—but to prevent the problem from developing in the first place.
BIBLIOGRAPHY
(1) Blumenthal RS, Morris PB, Gaudino M, Johnson HM, Anderson TS, Bittner VA, Blankstein R, Brewer LC, Cho L, de Ferranti SD, Gianos E, Gluckman TJ, Gradney KF, Isiadinso I, Lloyd-Jones DM, Marrs JC, Martin SS, McLain KH, Mehta LS, Mora S, Mulugeta WM, Natarajan P, Navar AM, Orringer CE, Polonsky TS, Reynolds HR, Saseen JJ, Shapiro MD, Soffer DE, Tynes SA, Villavaso CD, Virani SS, Wilkins JT. 2026 ACC/AHA/AACVPR/ABC/ACPM/ADA/AGS/APhA/ASPC/NLA/PCNA Guideline on the Management of Dyslipidemia: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J Am Coll Cardiol. 2026 Mar 13:S0735-1097(25)10254-4. doi: 10.1016/j.jacc.2025.11.016. Epub ahead of print. PMID: 41824590.
(2) Gráfico extraído del blog de https://peterattiamd.com/measuring-cardiovascular-disease-risk-and-the-importance-of-apob-part-1/