Adrenal fatigue (AF) goes through a series of phases as the body reaches an imbalance. It is the body’s reaction as it tries to return to a state of simplicity when it’s faced with a life that has become too complicated.
The Ovarian-Adrenal-Thyroid axis is vitally important to women and its role in adrenal fatigue. These 3 glands are intensely co-dependent for optimal functioning. When one of them suffers an alteration, either due to a pathology or medication, the other two may be affected, as well. In adrenal fatigue syndrome, cortisol produces a state of multiorgan resistance.
Dr. Alfonso Galán González – Neolife Medical TeamUnder chronic and severe stress, the adrenal gland is eventually not able to meet the demand for cortisol.
In this series of articles, my goal is to describe this entity known as adrenal fatigue syndrome. In the first part, we saw the symptoms that may arise and their causes. In this second installment, we will see how it evolves, the phases it may go through, and the symptoms and phenomena that determine each phase.
Adrenal fatigue goes through a series of phases as the body reaches an imbalance. It is the body’s reaction as it tries to return to a state of simplicity when it’s faced with a life that has become too complicated.
Phase 1: Reaction of Alarm
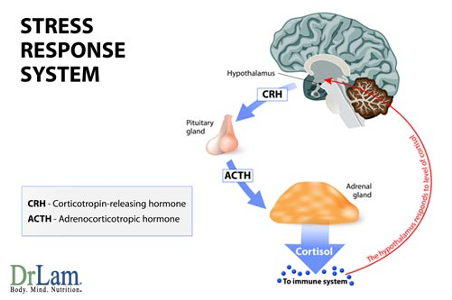
In this phase, the body goes into a state of alarm due to stressors and mounts an aggressive anti-stress response.
The pituitary gland releases ACTH, stimulating the adrenal gland to release epinephrine and cortisol. There is usually, but not always, a reduction in DHEA production. In this phase, there are no major symptoms. There may be a feeling of tiredness, but daily activities can still be carried out (1).
Phase 2: Resistance
Under chronic and severe stress, the adrenal gland is eventually not able to meet the demand for cortisol, and its production begins to decline from its previous high levels to more normal values, while ACTH remains elevated. The adrenal glands start to show signs of exhaustion. Anxiety appears and the person becomes irritable. Insomnia becomes more frequent, with difficulty falling asleep and staying asleep. The individual is more susceptible to infections. Premenstrual symptoms and menstrual irregularities appear in women, as well as symptoms that suggest hypothyroidism, like the inability to tolerate cold and a slow metabolism.
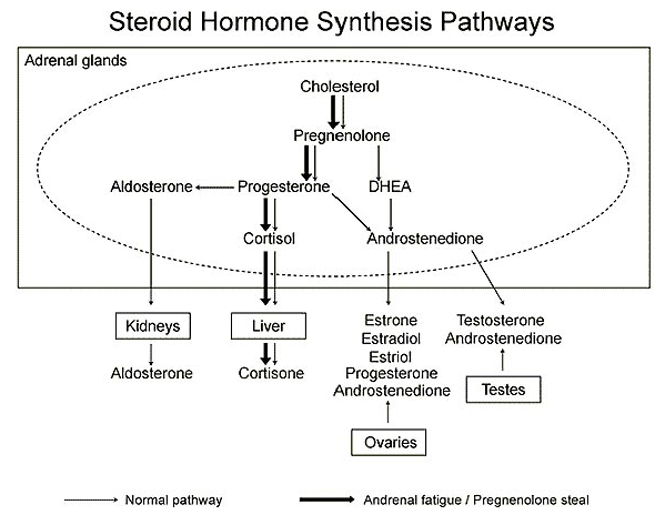
A phenomenon called “pregnenolone steal” occurs, in which the body favors the production of cortisol over that of other hormones, and consequently levels of DHEA, pregnenolone, estradiol, testosterone, progesterone, etc., drop. The daily production cycle of cortisol is altered and its usual morning increase is lost.
In this phase, you feel some fatigue that may be solved with a nap or a few days of rest.
Phase 3: Adrenal Exhaustion
Despite the increase in ACTH, the adrenal glands cannot maintain the pace of cortisol production that the body demands, and ultimately, its release is lowered, as well as DHEA levels. The body cannot maintain a state of equilibrium.
This phase can be divided, in turn, into 4 subphases, A, B, C, and D.
Initially, the symptoms of the previous two phases become more persistent and chronic (A). As it worsens, multiple hormonal imbalances occur due to the alterations suffered by the Ovarian-Adrenal-Thyroid axis (Adrenal-Thyroid in men). The body is in a state of constant mild to moderate fatigue (B).
Phase C is characterized by a reactive imbalance. The body tries to compensate by activating the autonomic nervous system and the adrenal marrow, producing adrenaline and norepinephrine in large quantities. Additionally, the other axes of the neuroendocrine metabolic system mentioned in the previous article are altered and trigger paradoxical reactions. Thus, we find: changes in blood sugar levels, fluctuations in blood pressure, postural hypotension, palpitations, postural orthostatic tachycardia, dizziness, anxiety, periodic adrenaline discharges, etc. (2). The connection between the mind and the body is very powerful and each thought carries with it a physiological reaction.
All hormone levels fall below the minimum needed to function normally, and no more of the hormones are secreted. The body enters a state of savings in which only minimal bodily functions are allowed. This state of quasi-failure is very serious. Individuals in this phase (D) are usually bed-ridden and need assistance in almost any aspect.
Phase 4: Failure
Phase 4 is indistinguishable from Addison’s disease (adrenal insufficiency). There is extreme fatigue, weight loss, muscle weakness, loss of appetite, nausea, vomiting, hypoglycemia, depression, dehydration, etc. Failure to treat may result in a fatal outcome.
Lab Tests
There are several lab tests available for adrenal fatigue, but unfortunately these do not present diagnostic value. Normal values do not rule out the disease.
The values of cortisol and DHEA give us a general idea of the state of the adrenal gland and whether we are facing an anabolic (tissue-building) or catabolic (destruction) state.
To increase accuracy, a serial determination of cortisol in saliva can be made 4 times during the day (8 a.m., noon, 5 p.m., and before bedtime). We observe the state of this curve, in other words whether it’s flat or at which points production is altered, and then we correlate it with the patient’s symptoms (3).
But, I repeat, laboratory values are only helpful. They may sometimes confuse rather than clarify. A good medical history compiled by a physician who possesses advanced knowledge and experience in this problem may prove more accurate.
Ovarian-Adrenal-Thyroid Axis
Let’s turn our attention now on this hormonal axis that is vitally important to women and its role in adrenal fatigue.
These 3 organs (or glands) are intensely co-dependent for optimal functioning.
When one of them suffers an alteration, either due to a pathology or medication, the other two may be affected, as well. For example, after administering thyroid hormone, a woman may experience menstrual disorders or stress intolerance.
In adrenal fatigue syndrome, cortisol produces a state of multiorgan resistance. Adrenal fatigue is usually associated with subclinical hypothyroidism or thyroid hypofunction, with laboratory values within the normal range, which confuses doctors and leads them to prescribe to their patients drugs for depression because they present a series of symptoms they are not familiar with, which only makes the problem worse (4).
Few hormones work properly in a state of adrenal fatigue. Insulin, testosterone, progesterone, estradiol, etc., may be affected. Their mechanisms of regulation and feedback don’t work, and their effects on the organs they target are erratic.
Let’s look at their relationship with the ovary (which under normal conditions produces estradiol, progesterone, and testosterone in women) (5). Many women, due to a stressful lifestyle, suffer from adrenal exhaustion in their late thirties or early forties. When too much cortisol is produced, this leads to multiple undesirable effects, In this case, it blocks progesterone receptors, and their production is compromised in favor of cortisol.
Insufficient progesterone levels lead to an imbalance between estradiol and progesterone, which in turn leads to symptoms of “estrogenic excess” or “estrogenic dominance”, such as premenstrual syndrome, fibroids, water retention, hot flashes, etc.
Specialists should proceed with caution when treating and replenishing the different hormonal axes in cases of adrenal fatigue.
In the next article in this series, we will provide ways in which adrenal fatigue may be treated.
BIBLIOGRAPHY
(1) Gadinger, M. C., Loerbroks, A. et al. Associations Between Job Strain and the Cortisol/DHEA-S Ratio Among Management and Nonmanagement Personnel. Psychosom Med. 2010;
(2) Chrousos, G. P. The role of stress and the hypothalamic-pituitary-adrenal axis in the pathogenesis of the metabolic syndrome: neuro-endocrine and target tissue-related causes. Int J Obes Relat Metab Disord. 2000; 24 Suppl 2:S50-S55.
(3) Matthews, K., Schwartz, J. et al. Diurnal cortisol decline is related to coronary calcification: CARDIA study. Psychosom Med. 2006; 68(5):657-661.
(4) Gur, A., Cevik, R. et al. Hypothalamic-pituitary-gonadal axis and cortisol in young women with primary fibromyalgia: the potential roles of depression, fatigue, and sleep disturbance in the occurrence of hypocortisolism. Ann Rheum Dis. 2004; 63(11):1504-1506.
(5) Heim, C., Ehlert, U. et al. Abuse-related posttraumatic stress disorder and alterations of the hypothalamic-pituitary-adrenal axis in women with chronic pelvic pain. Psychosom Med. 1998; 60(3):309-318.
Para ofrecer las mejores experiencias, utilizamos tecnologías como las cookies para almacenar y/o acceder a la información del dispositivo. El consentimiento de estas tecnologías nos permitirá procesar datos como el comportamiento de navegación o las identificaciones únicas en este sitio. No consentir o retirar el consentimiento, puede afectar negativamente a ciertas características y funciones.
Funcional
Always active
El almacenamiento o acceso técnico es estrictamente necesario para el propósito legítimo de permitir el uso de un servicio específico explícitamente solicitado por el abonado o usuario, o con el único propósito de llevar a cabo la transmisión de una comunicación a través de una red de comunicaciones electrónicas.
Preferencias
El almacenamiento o acceso técnico es necesario para la finalidad legítima de almacenar preferencias no solicitadas por el abonado o usuario.
Estadísticas
El almacenamiento o acceso técnico que es utilizado exclusivamente con fines estadísticos.El almacenamiento o acceso técnico que se utiliza exclusivamente con fines estadísticos anónimos. Sin un requerimiento, el cumplimiento voluntario por parte de tu proveedor de servicios de Internet, o los registros adicionales de un tercero, la información almacenada o recuperada sólo para este propósito no se puede utilizar para identificarte.
Marketing
El almacenamiento o acceso técnico es necesario para crear perfiles de usuario para enviar publicidad, o para rastrear al usuario en una web o en varias web con fines de marketing similares.