

Last May, The Lancet published the outcome of an unprecedented international consensus process: polycystic ovary syndrome (PCOS) will no longer be known by that name and will instead be renamed polyendocrine metabolic ovarian syndrome (PMOS). Led by Monash University and endorsed by the World Health Organization, this change is far more than a cosmetic adjustment in terminology; it is the result of fourteen years of scientific work.
Behind the new name lies an extensive process involving iterative global surveys, modified Delphi methods, and the participation of more than 14,000 individuals—both patients and healthcare professionals—from every region of the world. The goal was to identify a name that accurately reflects what is truly happening in the bodies of those living with this condition.
Dr. Carlos Martí – Neolife Medical Team
A new name to better reflect clinical reality
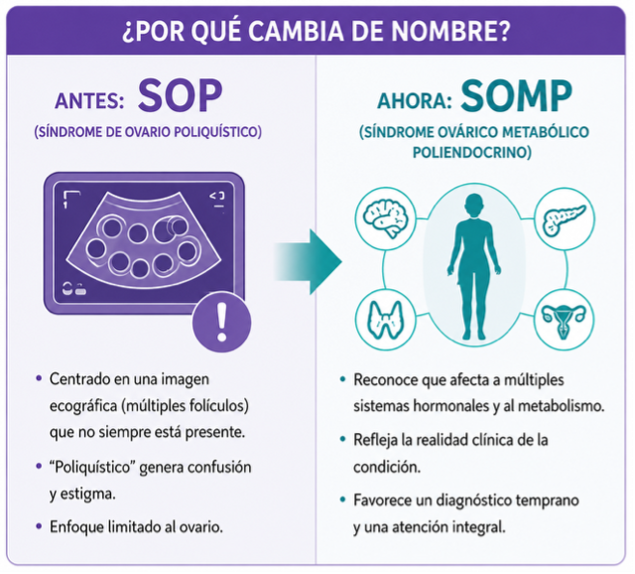
For decades, the term “polycystic” focused attention—and diagnosis—on a specific ultrasound finding: the presence of multiple follicles within the ovary. Yet these follicles are not pathological cysts, but rather immature structures that failed to complete their development, and many women with the condition do not even exhibit this ovarian morphology.
This discrepancy between the name and the clinical reality had important consequences: delayed diagnoses, fragmented care, and a stigma that remains associated with the word “polycystic.” The new name aims to put an end to this confusion and to acknowledge, from the terminology itself, that this is a multisystem disorder involving hormonal, metabolic, and reproductive dysfunction simultaneously.
The magnitude of the problem justifies the change. According to the WHO, PMOS affects one in eight women of reproductive age worldwide, and up to 70% of cases are estimated to remain undiagnosed. The transition to the new terminology will be implemented gradually over the next three years, with updates to clinical guidelines, diagnostic classifications, and educational materials for patients.
From PCOS to PMOS: the anatomy of a global consensus
The process, published on May 12, 2026, and led by Professor Helena Teede together with the Global Name Change Consortium, involved 56 academic, clinical, and patient organizations. The aim was not merely to select a new name based on the opinion of a few experts, but rather to build it upon scientific evidence and the real-world experiences of individuals living with the condition.
The new terminology was officially presented during the European Congress of Endocrinology in Prague and simultaneously published in The Lancet. According to the authors, the priority was to find a precise term, even if this meant leaving behind the familiar PCOS acronym that had defined the condition for decades.
The three pillars of the new name
The term polyendocrine metabolic ovarian syndrome encapsulates three key concepts.
“Polyendocrine” acknowledges that the disorder extends beyond the ovaries and involves multiple hormonal systems, including androgens, insulin, and, in some cases, thyroid function.
“Metabolic” places insulin resistance and cardiovascular risk at the center of the condition, rather than treating them as secondary complications.
“Ovarian” preserves the reproductive origin of the syndrome while removing the misleading reference to cysts.
This new terminology is not only more accurate; it also provides a better framework for treatment. A condition that simultaneously affects metabolism, multiple endocrine pathways, and the reproductive system cannot realistically be managed from a single specialty.
What is PMOS and how is it diagnosed?
Beyond the name change, PMOS continues to be diagnosed using the well-established Rotterdam criteria. At least two out of three conditions must be present:
Ovulatory dysfunction (irregular menstrual cycles or anovulation).
Excess androgen levels, either clinically (acne, hirsutism, hair loss) or demonstrated biochemically.
Characteristic ovarian morphology on ultrasound or elevated anti-Müllerian hormone levels.
In adolescents, diagnostic criteria are applied more cautiously, and only the first two criteria are considered.
These combinations give rise to different phenotypes; not all women with PMOS share the same profile. Some present with hyperandrogenism and irregular cycles together with polycystic ovarian morphology, whereas others exhibit the same hormonal abnormalities without the ultrasound findings. Still others maintain normal ovulation while showing androgen excess and multiple follicles. This variability is precisely what the new terminology aims to capture more effectively.
Although insulin resistance is extremely common in PMOS, it is not part of the formal diagnostic criteria. Nevertheless, it strongly influences prognosis and treatment, which explains why the metabolic component now occupies a central place in the disease’s name.
Why naming matters for health
Women with PMOS experience a wide range of manifestations: irregular cycles, difficulty conceiving, persistent acne, excessive hair growth, and hair loss, but also an increased risk of type 2 diabetes and cardiovascular disease. The previous terminology, focused mainly on the ovaries, tended to overlook these metabolic implications, which are often the most significant determinants of long-term health.
Accurately naming a disease is not merely symbolic. When terminology reflects the true complexity of a condition, it improves clinical recognition, accelerates diagnosis, and facilitates coordinated care among different specialties.
The cardiovascular component: why it is not a minor detail
Cardiovascular risk is not a secondary consequence of PMOS but one of the fundamental reasons behind the name change. Insulin resistance is present in approximately 85% of affected individuals and represents one of the central mechanisms driving the syndrome. Compensatory hyperinsulinemia stimulates ovarian and adrenal androgen production, reduces sex hormone-binding globulin (SHBG), and increases circulating free testosterone levels.
Ese mismo desequilibrio favorece la acumulación de grasa visceral y hepática, un estado proinflamatorio de bajo grado y disfunción del endotelio vascular, ingredientes que, sostenidos en el tiempo, derivan en hipertensión arterial, dislipemia y aterosclerosis prematura. El riesgo de diabetes tipo 2 y de diabetes gestacional también aumenta de forma proporcional al peso corporal.
For this reason, current guidelines recommend that all women newly diagnosed with PMOS undergo a metabolic evaluation including a lipid profile and an oral glucose tolerance test, regardless of age or body mass index. Early identification of these abnormalities allows intervention before overt cardiovascular disease develops, in line with the preventive approach that we apply at Neolife to cardiometabolic risk factors.
How PMOS is treated
Treatment of PMOS has never relied on a single solution, and this does not change with the new terminology. Management remains individualized and depends on the patient’s predominant symptoms, reproductive goals, and degree of metabolic impairment.
For most women, the first step consists of lifestyle interventions: adopting a diet that improves insulin sensitivity, engaging in regular physical activity, and achieving moderate weight loss when appropriate. These measures alone can improve menstrual regularity, reduce hyperandrogenism, and lower long-term cardiometabolic risk.
When metabolic dysfunction is significant, insulin-sensitizing agents such as metformin are often used. Combined hormonal contraceptives and antiandrogens are commonly prescribed to regulate menstrual cycles and manage acne or hirsutism, with spironolactone remaining one of the most widely used medications because of its effectiveness against excessive hair growth and acne. However, it should be avoided in women seeking pregnancy because of its teratogenic potential.
For women wishing to conceive, ovulation induction therapies such as letrozole or clomiphene citrate are available, and if necessary, assisted reproductive technologies such as in vitro fertilization may be considered.
Importantly, PMOS does not necessarily imply infertility. Many women with the condition achieve spontaneous or assisted pregnancies. The key lies in comprehensive follow-up involving gynecology, endocrinology, and nutrition, together with psychological support whenever necessary, given the emotional burden associated with living with a chronic condition.

What changes—and what does not—for patients
The symptoms do not change. A woman with PMOS experiences exactly the same manifestations previously associated with PCOS. What changes is the framework used to understand and integrate these manifestations into a single clinical picture, as well as the way healthcare professionals communicate and coordinate care.
The transition will be gradual. Over the next three years, clinical guidelines, classification systems, medical records, and educational resources for both patients and professionals will be updated. The goal of the consensus initiative is not to transform clinical practice overnight, but rather to ensure an orderly evolution toward this new diagnostic framework.
The Neolife approach
At Neolife, we have long approached female hormonal disorders through a comprehensive perspective, integrating endocrinology, gynecology, and nutrition to understand what happens beyond the ovary itself. This change in terminology reinforces something that has always been part of our clinical practice: evaluating each patient’s hormonal, metabolic, and reproductive profile as a whole, rather than treating individual symptoms in isolation.
Because giving a disease the right name is often the first step toward treating it better.
BIBLIOGRAPHY
(1) Teede HJ, Bahri Khomami M, Morman R, et al; Global Name Change Consortium. Polyendocrine metabolic ovarian syndrome, the new name for polycystic ovary syndrome: a multistep global consensus process. Lancet. 2026 Jun 6;407(10545):2329-2339. doi: 10.1016/S0140-6736(26)00717-8. Epub 2026 May 12.
(2) Teede HJ, Moran LJ, Morman R, et al. Polycystic ovary syndrome perspectives from patients and health professionals on clinical features, current name, and renaming: a longitudinal international online survey. EClinicalMedicine. 2025;84:103287.