


Irritable Male Syndrome is a type of depression with four distinctive features: exaggerated sensitivity, anger, frustration, and anguish.
Physiologically, as the main symptom of hormonal decline, men may experience erection problems sporadically, so if they connect their masculinity to their sexual performance, they may feel frustrated.
Dr. César Montiel – Neolife Medical Team
Andropause
First, we must clarify that the term “andropause” is not a male equivalent of menopause. We use it figuratively to refer to the deficit of free testosterone (T) in the adult. And secondly, we must distinguish between depression and dysthymia; although both are emotional disorders, they differ in severity and time elapsed, depression being the more acute and severe of the two.
Irritable Male Syndrome is a type of depression with four distinctive features: exaggerated sensitivity, anger, frustration, and anguish. Other common symptoms of depression linked to andropause are the following: hostility (with a lack of anger management), resentment (inability to forgive, but usually later regret), anxiety, anger, impatience, emotional flatness (fewer demonstrations of feelings), hopelessness, feelings of failure, taking refuge in television shows, temper tantrums, etc.
A clinician, urologist, endocrinologist, psychiatrist, or psychologist are duly trained to detect this clinical syndrome, or at least suspect it; likewise, the earlier the consultation is made, the greater the chances of preventing the progression of these symptoms and improving the patient’s quality of life. Here at Neolife, we have a specialized medical team to accompany the patient through this stage, and we also use the most advanced diagnostic tests.
From the age of 40 onwards, every man should be monitored for any physical or psychological elements (irritable male syndrome) linked to andropause, especially a decrease in sex drive and erectile quality. As soon as any of these characteristics are observed, it is time to schedule a consultation at NEOLIFE to begin effective control and the proper treatment of this phase, thus improving quality of life and continuing with a healthy sexuality and overall healthy life.
The treatment with testosterone in the Hormone Replacement Therapy that we offer at NEOLIFE is given to all patients with symptoms whose blood shows lower concentrations of this hormone, and as long as there are no contraindications such as prostate or liver disease among others.
The main male hormone, testosterone or androsterone, has long been considered to have antidepressant properties, although until recently, the mechanism of its occurrence was not known. It has recently been learned that there is an area in the hippocampus, which is an area related to memory, especially episodic and spatial, and stress response. It is in this area, located within the temporal lobe that connects to the cerebral cortex, where the active action of this hormone acts as a mediator.
Compared to men, women are twice as likely to suffer from depression and other mood disorders, which may explain why the number of women is 20 to 30 times lower. Depression and anxiety events are also common in adults with free T deficiency.
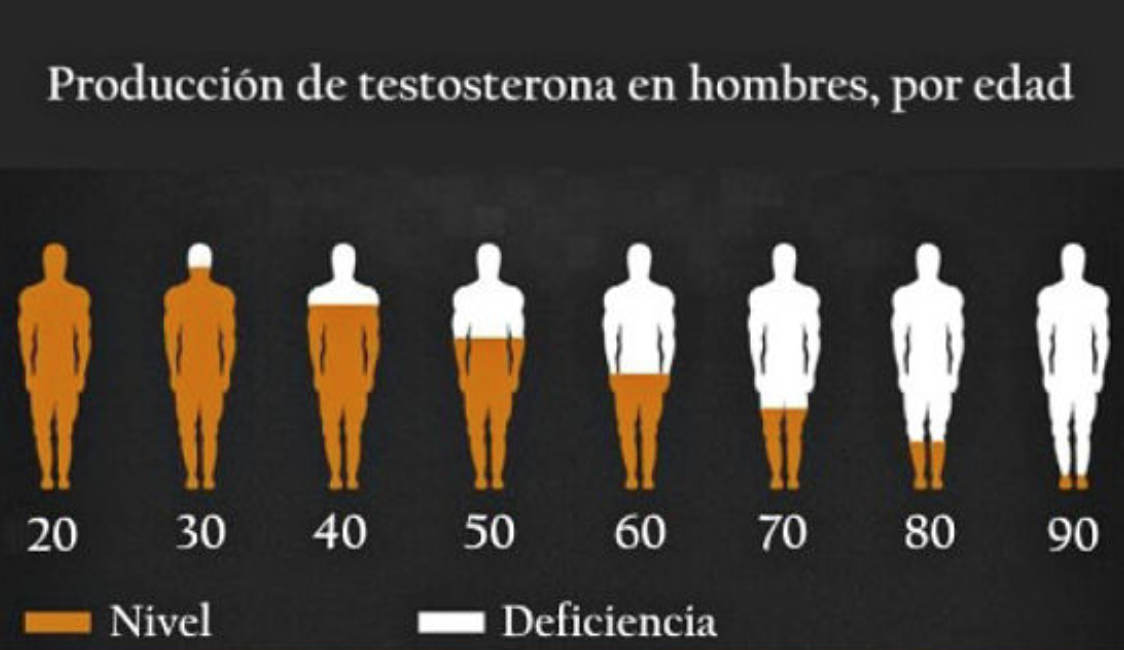
A molecular marker has been found to be essential for the male hormone to have the proper effect on mood, thus combating the recurrent sadness that can occur in these cases. We are talking about free testosterone. Values decrease by 1.6% annually after the age of 50; however, individual differences may exist. Total T values decrease by 35% in men between 20 and 80 years old, while free T decreases by 50%. (Figure 1)
It has been demonstrated that with age there is a loss of the circadian rhythm (night-day cycle) of Testosterone secretion in the older adult, as well as an elevation of SHBG (sex hormone-binding globulin), and constitutes the non-biologically active fraction. While only the remaining 2% circulates in free form to be used by the cells of the body.
SHBG levels increase with age, therefore, when there are higher concentrations of circulating SHBG there is less circulating free testosterone.
The most important symptoms of andropause are low sex drive, erectile dysfunction, low sperm count, sleeping problems; lower muscle strength and size; bone loss, increased body fat, and of course, emotional disorders (depression and problems concentrating…).
To explain all these symptoms a little bit, we could summarize it by delving into the cascading decrease of the following hormones, which occurs in this phase of male life. Dihydrotestosterone (DHT) is a metabolic product of Testosterone, is produced in the brain, skin and adrenal glands, and is the most abundant steroid hormone in the body. As men age, DHT concentrations decrease, and by the age of 45, DHT production is half that of a 20-year-old.
Dehydroepiandrosterone (DHEA) also decreases with increasing age in men; GH, insulin-like growth factor 1 (IGF-1) and melatonin concentrations decrease; while leptin (a hormone that controls hunger and satiety) values are increased, which could partly explain the changes found in body fat distribution.
The increase in adipose tissue, particularly abdominal adipose tissue, in older men is associated with an increase in the activity of the enzyme aromatase, which converts testosterone to estradiol (E2), resulting in a decrease in testosterone values and an increase in E2 values.
All this complex cascade of biochemical events will lead to a situation of hormone depletion, with the resulting psychological consequences.
And this may lead to or facilitate a mood disorder that may or may not be hidden, but if it manifests itself unequivocally, some of the symptoms will be the following:
- Altered mood or loss of interest or pleasure in almost all usual activities, with sadness, hopelessness or apathy, lack of initiative, and irritability.
- Lower sex drive, low energy, and fatigue. Feelings of worthlessness, self-reproach, or excessive or inappropriate guilt; lower ability to concentrate and indecisiveness.
- There may be weight loss and poor appetite or increased appetite with weight gain.
- In terms of quality of sleep, there may be insomnia or drowsiness.
Why isn’t this syndrome diagnosed?
It often goes undiagnosed in men for a number of reasons, among them:
Lack of awareness: You may think that feeling sad or emotionally unstable is always the main symptom, but for many men, it’s not. For example, headaches, digestive problems, fatigue, irritability, or long-term pain may sometimes be indicative. So can feeling isolated and seeking distraction to avoid dealing with feelings or relationships.
Minimizing signs and symptoms: You may not recognize how much your symptoms affect you, or you may not want to admit that you are not the same emotionally as before. But ignoring, suppressing, or masking the situation with unhealthy behavior will only worsen the negative emotions.
Refusing to talk: You may not be open to talking about your feelings with family or friends, let alone a doctor or mental health professional. Like many men, you may have learned to emphasize self-control. You may think that it’s not manly to express emotions and feelings.
Resisting mental health treatment: Even if you suspect there’s something wrong, you may avoid diagnosis or refuse treatment. You may avoid getting help because you are concerned that the stigma of possible depression or emotional disorder may hurt your career or cause your family and friends to lose their respect for you.
Is there anything we can do about it?
There isn’t much we can do to avoid suffering from this social syndrome since, at certain ages, the decrease of testosterone is something natural in men, as is the decrease of estrogen in women. However, at NEOLIFE, we can offer some tips to make irritable male syndrome as painless as possible:
- Medically monitor your hormones. In our check-ups, blood tests are the key to treatment, and we can also see if there are abnormally low levels of testosterone (hypogonadism) in the body, in which case, we can administer a replacement treatment to help reduce the symptoms.
- Learn to control your mood. Moodiness remains a defensive response to situations, words, or comments that you believe hurt you in some way. To learn to control your mood, you can do some introspection exercises to determine the origin of the anger, analyze your reactions, and make the commitment to redirect your energy in a positive way.
What is clear is that the effects of male hormones are significant on the patient’s mood, emotions, motivation, sleep quality, and overall mental processes. If a man is ready to accept that the bioidentical testosterone replacement we do at NEOLIFE is unavoidable and that he will have to take even more care of his physical exercise, diet, and lifestyle habits, he will continue to age but feel like the titan he has always been. The treatment requires periodic monitoring to check that testosterone levels are recovering adequately and to assess whether the patient is regaining his lost functions. And if the goal is to keep your libido and fitness in check, you will need to be consistent with your medication. If you stop, in a few months you will be right back where you started.
BIBLIOGRAPHY
(1) Wang C, Nieschlag E, Swerdloff R, Behre HM, Hellstrom WJ, Gooren LJ et al: Investigation, treatment, and monitoring of Late-Onset Hypogonadism in males: ISA, ISSAM, EAU, EAA and ASA recommendations. Eur Urol 2009; 55:121- 30.
(2) Buvat J, Bou Jaoudé G: Significance of hypogonadism in erectile dysfunction. World J Urol 2006; 24:657-67.
(3) Köhler TS, Kim J, Feia K, Bodie J, Johnson N, Makhlouf A, Monga M: Prevalence of Androgen Deficiency in Men with Erectile Dysfunction. Urology 2008; 71: 693–7.
(4) Martínez Jabaloyas JM, Queipo Zaragozá A, Gil Salom M, Chuan Nuez P: Evaluation of an immunoassay technique for the determination of free testosterone. Actas Urol Esp 2006; 30: 598-601.
(5) Mikhail N: Does testosterone have a role in erectile function? Am J Med 2006; 119: 373-382.